 Pilonidal Clinic
Pilonidal Clinic

Before the procedure
What to do about a Pilonidal Cyst before seeing a Doctor?
A pilonidal cyst, at any stage, can bring pain and discomfort that disrupt daily life. At first, the pain might be mild and occasional, but as inflammation grows


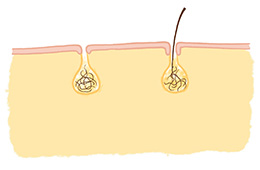
A pilonidal cyst is a chronic subcutaneous abscess located at the bottom of the intergluteal cleft. A characteristic feature is the presence of hair within the sinus cavity, though this is not always present.
Typical symptoms of a pilonidal cyst include (not all may be present simultaneously):
Learn more about pilonidal cysts:
Several theories explain the formation of pilonidal sinuses. The most likely involves skin damage at the bottom of a tight, deep intergluteal cleft due to sweat and mechanical abrasion. This leads to secondary infection of superficial wounds, followed by bacterial penetration into the subcutaneous tissue, resulting in an abscess cavity connected to the skin surface via one or more fistulous tracts.
Despite the common theory of ingrown hairs, studies indicate that hairs found in pilonidal sinuses are loose hairs detached from the skin and trapped in the intergluteal cleft, often originating from the scalp. Many are short, stiff hairs with sharp ends, such as those cut at a barbershop, which penetrate the sinus through damaged skin or fistulas.
If the issue is recent and you’re awaiting a doctor’s visit, you can try simple methods to feel better at home before receiving professional care. These are detailed on our blog:
Pain from a pilonidal cyst can be significant, especially with inflammation or purulent infection. Several methods can help alleviate pain before professional treatment. These are detailed on our blog:
The duration and course of recovery depend on multiple factors, including the type of procedure performed. Wounds from surgeries that do not involve flattening the intergluteal cleft may heal slowly or not at all, particularly if located between the buttocks with limited air exposure, preventing fluid evacuation. Wounds from procedures like the Bascom Cleft Lift, which flattens the cleft, typically heal quickly (2–3 weeks).
During healing, mild skin erythema is normal, but wound edges should remain soft and non-painful. Serous discharge (clear or slightly yellowish watery fluid) is part of the natural self-cleansing and healing process and is not concerning. However, if signs of inflammation appear—such as swelling, significant erythema, buttock induration, pain, or thick, white, or gray-brown malodorous pus – contact a nurse or physician.
Various treatment methods for pilonidal cysts differ in wound healing speed, post-operative quality of life, and recurrence risk.
Learn more about treatment planning and method selection on our procedures page:
A drain is a thin tube placed in the surgical wound to reduce discomfort, infection risk, and promote healing. Drainage typically lasts 5–10 days, though this varies individually. At Pilonidal Clinic by VenoMedica, we recommend drain removal for Bascom Cleft Lift patients when daily fluid output falls below 20 ml. Drains can be removed at home following instructions:
The purpose of a dressing is to protect the surgical wound from bacterial contamination and external factors like sweat or clothing fibers. Dressing changes and wound care continue until healing, typically 10–14 days.
Watch an instructional video on proper dressing changes after a Bascom Cleft Lift:
Most patients resume daily activities the day after surgery. After about two weeks, once the drain is removed and adhesive strips fall off, the wound is typically fully healed, allowing a return to normal life.
However, the scar continues to strengthen up to six weeks. During this time, avoid activities that could injure the buttock area, such as falls, impacts, contact sports or long sopking (swimming pool, bath tube).
Most patients resume daily activities the day after surgery. However, to avoid dislodging the drain or wound dehiscence, it’s sometimes better to wait until the drain is removed (5–10 days) before returning to work or school. The scar continues to strengthen for six weeks, during which activities risking buttock injury (e.g., falls, impacts, contact sports) should be avoided.
Surgery can be performed while on antibiotics, but the decision depends on several factors, including the reason for antibiotic use (whether related to the pilonidal cyst or another condition) and the patient’s overall health. If fever, chills, or other systemic inflammatory symptoms are present, surgery may be postponed until the patient’s condition stabilizes. Decisions are made individually, prioritizing patient safety and comfort.
Pilonidal cyst surgery is performed under tumescent anesthesia, a type of local anesthesia involving the slow injection of a large volume of diluted anesthetic into the tissues around the surgical site. This effective method provides pain relief for several hours post-procedure, allowing patients to leave the facility immediately after surgery.
Some patients experience minimal pain that resolves within the first 2-3 days, while others may have discomfort for longer, particularly those with higher pain sensitivity or after more extensive procedures. Post-operative pain is typically transient. If needed, patients can use analgesics to manage discomfort, though approximately 80% of patients report no need for pain medication.
Simple excision of a pilonidal cyst is often insufficient, as recurrence is likely without addressing risk factors. The primary modifiable factor is the depth of the intergluteal cleft. Flattening the cleft, as in the Bascom Cleft Lift, reduces recurrence risk to below 5%. Methods that do not address cleft depth have a higher recurrence risk, up to 50% in some cases.
While the surgical method is the primary factor influencing recurrence risk, lifestyle also plays a role in recovery and prevention. Post-operative care includes:
In the SiLaT laser treatment, small openings remain visible on the skin, but beneath the surface, a large cavity is left after the cyst walls are removed. This cavity takes approximately 4–6 weeks to close.
You can find a full explanation on the blog:
Shaving with a disposable razor can cause skin irritation in the intergluteal cleft area, so if a patient opts for hair removal, laser hair removal may be a safer method. Removing hair from the intergluteal cleft can facilitate proper hygiene, but its impact on a pilonidal cyst is difficult to predict and likely minimal. There are no studies confirming the effectiveness of this approach, so it is not considered an essential part of treatment.
In the event of a blocked drain, the only appropriate course of action is its removal.
Attempts to manually clear the drain should not be made, as this is ineffective and may lead to complications.
After drain removal, monitor the wound area. If concerning symptoms such as swelling, skin tension, or suspected subcutaneous fluid accumulation occur, contact the nurse responsible for postoperative care.
